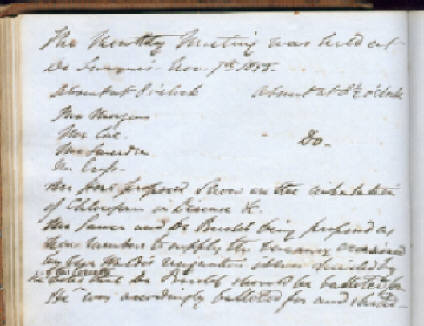
The Medical Reading Society of Bristol was founded by 11 Bristol doctors in March 1807, "for the purpose of promoting medical knowledge and a friendly intercourse among its members, and for purchasing medical books". This was some 24 years before there was a medical library in the city. It soon elected a 12th member and has never had more than 12 members at any one time. With a few exceptions it has met monthly since its foundation. This month it is celebrating its 200th anniversary. 1807 was also the year that the slave trade abolition act was passed; Bristol of course had made much of its wealth from the slave trade. My interest in this topic of Anaesthesia, Cholera and the Medical Reading Society of Bristol was aroused in November 2005 when I was looking at the minutes from 50 years, 100 years and 150 years ago, which are read out at our meetings, and came across this:
The monthly meeting was held to Dr Swayne's house on November 7, 1855. Absent at 8 o'clock. Mr Morgan, Mr Coe, Mr Smerdon and Mr Cross. Absent at 81/2 o’clock ditto-
Mr Hore proposed
Snow on the inhalation of Chloroform in Disease, etc.
Mr Sawer and Dr Budd being proposed as new members to supply the vacancy occasioned by Mr Waldo's resignation, it was decided by the votes of the Society that Dr Budd should be balloted for. He was accordingly balloted for and elected.
I was quite excited by this because, although John Snow had long been a hero of mine, I did not recognize the pamphlet mentioned here. So I sent an email to the secretary of the John Snow Society in London and also one to one of the authors of the definitive biography of John Snow. I did not realise quite what a reaction I would get. In the next five days I received 11 e-mails from various parts of the United Kingdom and America, including one that described the minutes of the Society as a historical treasure. I discovered that professors of history in Michigan knew far more about Bristol physicians of the 19th century than I did. They also told me that between 1848 and 1851 John Snow had written 19 articles On Narcotism by the inhalation of Vapours for the London Medical Gazette and these were later published as three separate pamphlets. The second contained parts 8 to 16. Part 8 was specifically about the actions of chloroform in disease states. This was the pamphlet that Mr Hore, who was the newest member of the Society, had proposed, but which was not actually purchased by the Society. I wonder why not. We know the Society took the London Medical Gazette for 10 years from 1927, but it was not currently taking it in 1855. However, by this time there were other medical libraries in the city, and it may well be that members had already read these articles.
The host Joseph Griffith Swayne was physician obstetrician at the Bristol General Hospital. When he was appointed in 1853 it was on the understanding that he would not undertake any surgery, though this restriction soon lapsed. He had a great interest in analgesia/anaesthesia in labour and he was also involved in the cholera story.
Another member present was Dr Fairbrother. In 1846 he was a physician to the Bristol General Hospital, and it was he who instigated and helped at the first anaesthetic given in Bristol, probably on the 31st of December 1946, possibly the 1st of January 1947, some 11 weeks after Morton's original demonstration in Boston in October. The surgeon was James Goodall Landsdown. The patient was a young man who underwent left above knee amputation. William Herepath, a professor of chemistry at the University provided the ether, and administered it at first, and then Alexander Fairbrother administered it a second time. Lansdown reported the Lancet in December 1847 that by then he had used ether 111 times including 30 during labour, one intermittent etherisation lasting 11 hours. However he went over to using chloroform enthusiastically soon after Simpson had published details of its use.
In 1853 Fairbrother resigned suddenly from the Bristol General Hospital and later became a physician at the Royal Infirmary.
We do know that no anaesthetics were given at the Bristol Royal Infirmary until August 1850, when chloroform was used. The six surgeons on the staff all signed the Surgical Consultation Book to say they had agreed jointly that chloroform should be given. Even then there was a nine-month gap before the second anaesthetic. As we shall see later at least one of the surgeons at the Infirmary was well informed about anaesthesia, and yet there is no explanation as to why they did not try it out.
Mr William Francis Morgan was one of the six surgeons at the Infirmary, as was Mr Augustin Prichard who was there that evening, but as he had not been appointed until 1850, he cannot be blamed for the delay in introducing anaesthesia there, though certainly he was suspicious of anaesthesia throughout his career.
Now we come to John Snow and William Budd. Born within two years of each other they were men of very different background, personality and lifespan, though both were acutely aware of how little treatment had to offer for the various fevers that ravaged the country in the 19th century and how vital it was to unravel the mode of transmission of these diseases to prevent them occurring.
William Budd has been described by his biographer, Michael Dunnill, as Bristol's most famous physician. He was born in 1811 into a large Devon medical family; his father and five of his brothers were also physicians. During his training in medicine William spent three separate years in Paris, interrupted by his catching typhoid fever. He qualified at Edinburgh as a doctor of medicine and won a gold medal for his thesis. In 1841 he moved to Bristol and became a consulting physician to the Bristol Royal Infirmary in 1847. He was a genial, vivacious, ebullient man, fond of good food, good wine and female company. An enthusiast in his work he could sometimes be seen running from his home in Park Street to the Infirmary so that he could see more quickly how his patients were getting along. His interest in epidemiology led him to play an active role in the development of the Bristol Water Company. Apart from his pioneering work on cholera, 1849, he described the contagious nature and prevention of Diphtheria, 1861; Anthrax, 1862; Tuberculosis, 1867, Scarlet Fever, 1869, and he also studied cattle plague and sheep smallpox. He is perhaps most renowned for his work on the waterborne transmission of Typhoid 1873. He died when he was 69 having suffered a stroke six years earlier, which had left him hemiplegic.
In contrast John Snow was the son the eldest son of a Yorkshire coal yard labourer. At the age of 14 he was apprenticed to Dr Hardcastle in Newcastle upon Tyne. He first met cholera in 1831 when at the age of 18 he was caring for miners at Killingworth colliery, before moving to York. From the age of 17 he was obsessed with the notion of pure water and at 23 gave a public address in which he suggested the numerous stills scattered around the country would be better put to producing distilled water than spirits. In 1836 he moved to London visiting Liverpool en route, and he walked from Liverpool to London via North and South Wales. In London he lived a frugal life as a bachelor, and was teetotal and a vegetarian. In addition to his pioneering work in on the transmission of cholera, after the discovery of anaesthesia in 1846 he rapidly became the foremost anaesthetist in the British Isles if not further afield. He was certainly the first anaesthetist to approach the subject in a scientific manner. He suffered from nephritis and at one time consulted Richard Bright. He died of a stroke at the age of 45, curiously enough attended in his final illness by William Budd's elder brother George.
Table 1. Members of Medical Reading Society October 1846, when the successful public demonstration of anaesthesia by William Morton took place in Boston, Massachusetts.
Years of membership
Mr William Mortimer 1807 - 1850
Mr John Estlin 1807 - 1855
Mr John Swayne 1807 - 1847
Mr William Goodeve 1820 - 1858
Mr Isaac Leonard 1823 - 1859
Mr William Morgan 1825 - 1873
Mr Charles Smerdon 1835 - 1870
Mr George Hetling 1838 - 1848
Dr Alexander Fairbrother 1839 - 1876
Mr John Colthurst 1844 - 1856
Mr Augustin Prichard 1844 - 1876
Dr Joseph Swayne 1845 - 1858
Notice that there were still three of the Founder Members still there in 1846 and that despite the predominance of surgeons it was Dr Fairbrother who instigated the first anaesthetic in Bristol.
|
|
|
|
|
Purchased |
Title |
Proposer |
|
1847 Oct |
Snow J . On the Inhalation of the Vapour of Ether in Surgical Operations.London: Churchill, 1847 |
Mr Morgan |
|
1848 Mar |
Curling TB The Advantages of Ether and Chloroform in Operative Surgery, London: Highley, 1848. |
Mr Morgan |
|
Oct |
Simpson JY. Answer to religious objections to the use of chloroform in midwifery. Edinburgh: Sutherland & Knox, 1847. |
Dr Swayne |
|
Oct |
Protheroe Smith Scriptural authority for the mitigation of the pains of labour, by chloroform and other anaesthetic agents. London: Highley, 1848. |
Dr Swayne |
|
Oct |
Merriman S. Arguments against the indiscriminate use of Chloroform in Midwifery. London: Churchill, 1848. |
Dr Swayne |
|
1855 |
Murphy EW. Chloroform: its properties and safety in childbirth. London: Wilson and Maberley, 1855. |
Dr Swayne |
|
1858 |
Snow J . On Chloroform and other Anaesthetics, ed. Richardson BW. London: Churchill, 1858. |
Dr Budd |
Thomas Blizzard Curling was Lecturer on Surgery at the London Hospital. His pamphlet was based on a lecture he had given to the Hunterian Society in February 1848. In it he reflected on pain and how different people responded, including a few remarkable people who allowed surgery to take place without any complaint. I guess that this was the effect of adrenaline rather like people don't feel pain when they are mauled by a tiger. Overall Curling was very enthusiastic and optimistic about the place of anaesthesia, noting in particular the usefulness of the relaxation produced particularly when reducing dislocations and also that the death rate following amputation was lower in those patients who had been anaesthetised than in those who had not. However he did caution that ‘the administration of anaesthetic agents should be entrusted to a person, who by practice, has acquired a nice perception of their action and the full knowledge of their powers and varying effects, so as to be able to produce and maintain their influence to a proper degree’.
Protheroe Smith was an eminent London obstetrician. He strongly supported Simpson. He actually gave himself some chloroform rectally and found himself sometime later unconscious on the floor. Unfortunately rectal irritation and severe diarrhoea meant this was not a convenient form of administration.
Samuel Merriman in his Arguments against the indiscriminate use of Chloroform in Midwifery takes the line that nature can cope with labour better than people who intervene. He points out how the mortality of women in childbirth has declined and now is only one in 113. He says interventions such as forceps and ergot and anaesthesia are used too early and that pain, even severe pain, never actually killed anyone, and before using chloroform they should be sure that the risks were not greater than those of leaving the pain untreated. He refers to his esteemed friend Doctor Snow and says Snow’s papers on the use of anaesthetic vapours should be studied by all who propose to employ them medicinally.
In Chloroform its properties and safety in childbirth Murphy discusses the properties of chloroform and the opposition to its use. He reports that deaths from chloroform had all occurred in surgical cases, 30 deaths in 9000 cases, and none had occurred in labour. There had been one death in an obstetric patient occurring one and a half hours after delivery when there had been sudden dyspnoea and death from an unknown cause. This was the mother's fourth labour and it had been long and tedious due to a narrowing at the diameter of the pelvic cavity. Long forceps delivery had been necessary. Recovery from anaesthesia had been speedy and perfect. I wonder if this actually was a case of Mendelssohn's syndrome, which is exudative pulmonary oedema due to aspiration of gastric juice. If it was then it was not so much a chloroform death as an obstetric anaesthetic death. He also describes a mouthpiece and box for the administration of chloroform, and sets out 10 rules for its safe use.
On the mechanism of action of chloroform and other anaesthetics was John Snow's final paper on anaesthesia and was not actually published until after his death from stroke at the age of 44 years. It summarises both theoretical and practical considerations. Again it is one of the classics of anaesthetic literature. At post-mortem Snow's kidneys were shown to be small and contracted. He had earlier consulted Richard Bright and curiously enough was attended in his final illness by William Budd's elder brother, George. Incidentally around this time the society bought two books by George, one on diseases of the stomach and another on diseases of the liver.
Ellis’s On the safe abolition of pain in labour and surgical operations by anæsthesia with mixed vapours describes anaesthesia using different mixtures of alcohol, chloroform and ether at various times during the anaesthetic to improve the quality and safety anaesthesia. A.C.E as it was called remained intermittently in use until 1920s.
In 1958 there was a death in Bristol due to chloroform and Augustin Prichard reported it in the British Medical Journal. John Snow commented and incidentally reminding Prichard that a death had occurred in Bristol in 1854. He also said that if chloroform was a problem why not go back to using ether? In his final letter Augustin Prichard wrote:
I venture to prophesy that anaesthetics will more and more fall into disuse and will ultimately be had recourse to only for the most severe or protracted operations
Snow disagreed strongly and pointed out that Guy's and St Thomas's hospitals which were very slow to take up anaesthesia were the very places where deaths had occurred before those hospitals that were using it more regularly. Prichard would no doubt be interested to hear that there were over 3.5 million anaesthetic given in United Kingdom last year. You can read more about this exchange of letters in a paper by Robin Weller.
Table 3. Pamphlets on cholera bought by the Medical Reading Society 1832-1856
|
Purchased |
Title
|
Proposer |
|
1832 |
Lawrie, James.
Essay on Cholera founded on observations of the disease in various parts of India and in Sunderland, Newcastle and Gateshead.
Glasgow: Smith and son, 1832
|
Dr Swayne
|
|
1833 |
Hancock, John
. Observations on the origin and treatment of Cholera and other pestilential diseases, and on the Gaseous Oxide of Nitrogen as a remedy in such diseases, etc..
London, 1831.
|
Mr Estlin |
|
1833 |
Kennedy, James.
History of the Contagious Cholera; with remarks on its character and treatment in England 3rd ed.. 1832, Moxon,London,
|
Mr Estlin |
|
1833 |
L’Académie de Médicine.
Rapport sur le Cholera Morbus
Paris 1831
|
Mr Prichard |
|
1848 |
Parkes, Edmund.
Researches into the pathology and treatment of the Asiatic or Algide cholera.
London: Churchill, 1847
|
Mr Prichard |
|
1849 |
Scot, William.
aaren't go to sleep are on the
Report on the Epidemic Cholera as it appeared in the territories subject to the Presidency of Fort St George, abridged from the original report printed at Madras in 1824 with introductory remarks by the author.
Edinburgh: Blackwood; London: Murray,1847
|
Mr Colthurst |
|
1849 |
Parkin, John.
On the antidotal treatment of the Epidemic Cholera,
with a sketch
of the physiology of this disease, as deduced from that of intermittent fever
.
London, 1846
|
Mr Goodeve |
|
1856 |
Simon, John.
Report on the Last Two Cholera Epidemics in London, as Affected by the Consumption of Impure Water
. London: HMSO 1956
|
Dr Budd |
I could only find James Kennedy’s History of the contagious cholera, 3rd ed. in the Wellcome Foundation library in London, though the full text of the 2nd edition, published earlier the same year, available online and this describes in detail the spread of cholera within the country. Kennedy thought cholera could occur in any climate, but that it was contagious only to those who are predisposed to get it, i.e. he was a contingent contagionist. The 3rd edition has an extra section dealing with treatment Kennedy felt bloodletting was the mainstay, but he reported that two German physicians working in St Petersburg had given a salt solution, two tbsp of common salt in 6 oz of hot water, with further smaller doses, to 30 patients all of who had recovered. As they had bled the patients before giving the saline Kennedy felt that the bleeding might well have been the treatment that had succeeded. He also commented on a report by Dr Steevens in the Lancet about the successful treatment of 226 men with cholera at Coldbath Fields Prison. Dr Steevens had used a mixture of ½ drachm of carbonate of soda, 1 scruple of muriate of soda, 7 grains of chlorate of potash in a tumbler of water. There had only been 26 deaths. Kennedy was also unconvinced by this report and said that saline draughts could never be more than a humble accessory to other forms of treatment. Clearly though we have here two examples of 1830' s Dioralite. He also discusses the use of intravenous saline. With it Dr Latta of Leith turned a moribund woman into a jocular one within an hour, but sadly she died later. Lawrie, see above, tried it on six patients in Glasgow but had no success. In Edinburgh they used a solution of 120 grains of common salt, 40 grains of carbonate of soda, in 5 lbs and water heated to 110/115°F. They gave up to 40 lbs of this solution in two days and noted that ‘rigor was apt to follow’. In all cases there was an immediate improvement but then ‘reaction fever’ leading to death would follow. Other forms of treatment at this time included emetics, blistering, rubbing with hot towels, opium, calomel, purgatives, brandy, stimulants and even fluid restriction.
After the great epidemics in India cholera became endemic there it began to spread outward. When it invaded Eastern Europe in 1830, France sent four commissions to observe the disease in Poland and Russia, two of them sponsored by the Academies of Sciences and of Medicine. In June 1831 cholera was added to the list of importable diseases, but in July L’Académie de Médicine in its Rapport sur le cholera morbus provisionally declared the disease not essentially contagious, but able to become so, and advised the government to take both sanitary and hygienic measures. When the epidemic arrived in 1832 it was catastrophic; in Paris alone 18,000 died. Medical remedies proved as futile as quarantines. Worse, the calamity signaled the breakdown of public order in France.
An abridged version of Scot’s 1924 report was published in 1831 and then again in 1849. In his introductory remarks in 1849 he says that the mortality from cholera continued to be as great, opinions even more unsettled, rules of practice as undefined, men's minds as much adrift as ever. He thought dysfunction of the ganglionic system of nerves formed the primary seat of the disease. He recognized that bodies of men travelling through the country could catch the disease while passing through affected areas and then carry cholera along with them. He discussed the role of the rivers, which were generally thought to have a great influence on the prevalence and intensity of cholera. However he says Dr Lorimer reports that out of 121 outbreaks only 37 occurred on the banks of rivers and he comments that cities are built on rivers, which are the lowest, and often most squalid, parts of any city. In the UK cholera clearly is an imported disease. He discusses treatment by opium, calomel, bloodletting and stimulants. Bloodletting might be all right on general principles early in the disease, but in the collapsed patient it was often deleterious.
Dr. John Parkin is something of an enigma. In 1832 he had suggested using a charcoal as a water filter, because he thought the cholera poison, having been generated in the earth, found its way into various springs and then into the stomach. Later he became a fanatical opponent of the water-borne theory and ridiculed the suggestion that cholera was caused by a living organism. In his 1846 paper he claimed to have a specific remedy, namely carbonic acid gas, to prevent collapse in cholera patients. He mixed 30 gr sesquicarbonate of soda or potash, 20 gr citric or tartaric acid, 1½ wine glasses of water and 1 dessertspoonful of syrup. This was given every 15 minutes for the first hour; less often thereafter. Fluids were allowed as the patient wished. Sesquicarbonate is a naturally occurring mixture of carbonate and bicarbonate. So what Parkin was actually doing was giving alkali therapy with fluids and plenty of sodium or potassium, a 1840s dioralite. In a collapsed apnoeic patient sodium bicarbonate therapy can be very harmful because carbon dioxide can diffuse readily into the cells and add to the acidosis. Here however the patient is getting rid of carbon dioxide by burping and he is also able to breathe it out. I guess this treatment is not as bizarre as it first sounded. The syrup was added to stop the carbon dioxide gas bubbling away before the patient had swallowed the medicine, because Parkin thought this was the active agent.
Before I tell you about the last pamphlet bought by the Society I need to refer to three papers that it did not purchase. In September 1849 John Snow published his pamphlet On the mode of communication of cholera and this was followed 29 days later by William Budd’s Malignant Cholera: Its Mode of Propagation and Prevention. The two men agreed that cholera was a disease of the gut, that other features were from dehydration and that water contaminated with cholera evacuations was a major source of spread. They disagreed in that Budd thought transmission by inhalation was feasible and that the causative agent was a fungus, one that had been identified by Joseph Swayne and his colleague Dr Frederick Brittan, who later became a member of the Reading Society. Budd was always meticulous in giving priority to Snow.
In 1954 John Snow had the opportunity of further studies on cholera, especially those where he related deaths from cholera to houses with piped water supplies from different water companies, or alternatively houses who got their water from different pumps, especially during the epidemic in the neighbourhood of Golden Square. Beside those who questioned whether Snow’s theory was true were those who said it wasn't original. Snow however had approached the matter in a scientific manner and had produced substantial statistical evidence to support his theory.
The last paper on cholera the Society bought was by John Simon, the first Medical Officer of Health in London, reporting to the General Board of Health in 1856. However he did not acknowledge Snow's work, of which his own was corroboration and an extension. At a meeting of the British Medical Association in Manchester later in the year Budd strongly supported a motion of regret at this omission, once again giving Snow the priority.
Finally I strongly recommend to you the recent biography of William Budd by Michael Dunnill, who was a medical student in Bristol in the 40s and who feels William Budd's worth has been inadequately recognized. Bruce Perry in his list of the ten most important doctors in Bristol fails to mention Budd. It will only cost you £12.99, and is a fascinating read. The biography of John Snow, see below, is also a splendid and scholarly book.
Michael Dunnill. Dr William Budd, Bristol's most famous physician ,. Bristol: Redcliffe Press, 2006.
Vinten-Johnansen P., Brody H., Paneth N., Rachman S., Rip M. Et al. Chloroform, Cholera, and the Science of Medicine, a Life of John Snow. Oxford: University Press, 2003.
Munro Smith G. A History of the Bristol Royal Infirmary. Bristol: Arrowsmith, 1917.
Odery Symes, J. A Short History of the Bristol General Hospital. Bristol: Wright, 1932.
Bennet JA. The eclipsed dawn of anaesthesia in Bristol. The History of the Anaesthesia Society Proceedings, 1999; 25: 85-89.
Weller R. The first general anaesthetic in Bristol. The History of the Anaesthesia Society Proceedings, 1999; 25: 80-84.
Weller R. Death in Bristol. An exchange of views between Augustin Prichard and John Snow Anaesthesia, 1976; 31: 90-96.
Stratmann L. Chloroform, the Quest for Oblivion. Stroud: Sutton, 2003.
Griffiths LG. The Medical Readng Society. Brist Med-Chi J. 1907,XXV.97:222-23.
Appendix A
Books proposed by William Budd at the Medical Reading Society
1855 Transactions of the Pathological Society lst vol*
1856 Polarized Light 2nd ed Pereira
Pathology of Urine Heller
Present state of the theory and practice of medicine* Bennett
Lecon’s de physiologie experimentale appliquée à la
Médecine, nos. 1 and 2 Bernard
Physicians and Physic Simpson
Report on last two cholera epidemics in London Simon
Gazette médicale
1857 Sewerage of London and other large cities Copland
L’histoire de le decouverte de la circulation du sang Flourens
Chemistry of wine Mulder
1858 La vie et l’intelligence Flourens
Papers on the health of the people a blue book
On chloroform and other anaesthetics Snow
Researches on epilepsy Braun-Séquard
Archives de physiologie normale et pathologique1,2,3 Braun-Séquard
Transactions of the Odontological Society
1859 Yellow fever* Pym
Seaside Studies Lewes
1860 On the classification and geographical distribution of the Mammalia Owen
Report on yellow fever at Lisbon* Lyons
Palaeontology Owen
L’annee scientifique et industrielle 1859 Figuier
L’Institut
L’Heterogenie Pouchet
1861 Clinique Médicale 1st vol Trousseau
Sur la Societé Anthropologie vol 1 Merm
1862 Transactions of the Epidemiological Society
Natural History Review from start of new series ( WB to buy at half price)
Meteorology Herschel
Scientific Essays Holland
Popular Science Review
1863 Emphysema and Bronchitis Waters
Australian Climate and its influence in prevention and arrest of consumption Palmer
1864 Horses of the Sahara Daumas
Map of Geographical Distribution of Disease Johnstone
1865 Trichines a l'usage des medecins et des gens du monde Virchow
Gazette Medicale
1867 Report upon the epidemic at Maplewood Young Ladies Institution Palmer
1868 Cattle Plague Gamgee
Lecons sur la physiologie generale et comparee du systeme nerveux Vulpian
1868 Variation under domestication* Darwin
Revue des deux Mondes
Criminal Abortion Storer
William Budd
� Born 1811 North Tawton, Devon
� Father: retired naval surgeon, general practitioner, North Tawton
� Faculte de Medicine de Paris, 1828-29, 1833-34 and 1836-37
� Edinburgh University, 1837-38, gold medallist
� Moved to Bristol 1841
� Lecturer to Bristol Medical School, 1842-55
� Physician to St Peter's Hospital, 1843-47
� Physician to Bristol Royal Infirmary 1847-62
� Malignant cholera: its mode of propagation and its prevention, 1849
� Director of Bristol Water Co., c. 1850
� Medical Reading Society, 1855-69
� Describes the contagious nature and prevention of Diphtheria, 1861; Anthrax, 1862; Tuberculosis*, 1867: Scarlet Fever, 1869; also studied cattle plague and sheep smallpox
� Gave evidence to the Sanitary Commission, advocating the establishment of a Public Health Service, 1871
� Elected FRS, 1871
� Typhoid fever: its nature, mode of spread and prevention, 1873
� Died 1880, hemiplegic for his last six years
William Budd Health Centre; Blue Plaque 89 Park St.; Ward at BRI
Appendix B
To read LG Griffiths's paper on the first 100 years of the Society click here
I have received help from many people but I am particularly grateful for help in obtaining material to Louise Bruton of the medical library in Bristol, Leslie Greig and her staff at Southmead, Julianne Simpson of the Welcome Foundation, Clive Hurst of the Bodleian library, and Trish Willis, archivist at the Association of Anaesthetists. My thanks to you all.
Joseph Swayne
1819 - 1895


Nathaniel Smith, Henry Clark, Thomas Green and John Harrison, who were the other surgeons who signed the agreement to use chloroform at the Infirmary in 1850. All but Clark were members of the Reading Society at one time or another. Smith was one of the founder members.
Anaesthesia, Cholera and the Medical Reading Society of Bristol
Alexander Fairbrother
1809 - ?
Augustin Prichard
1818 - 1898


Boston Oct 16th 1846
Painting by Robert Hinckley



Snow's 1847 temperature controlled vaporiser and facemask
In this 16th century woodcut Adam appears to be supporting his own chin. God is working here as an operator/anaesthetist, which would be severely frowned on today
Agnes Anaesthesia Carstares, who 17 years earlier had been the baby born to the first mother to whom Simpson had given chloroform.
Simpson's chloroform bottle


Edmund Parkes 1819 - 1876
James Lawrie 1802 - 1859
John Snow 1813 - 1858
Thomas Curling 1811 - 1888
James Young Simpson 1811 - 1970

Sir John Simon 1816 - 1904
William Budd 1811 - 1888


William Morton 1819 - 1868